Every so often, you come across a treatment planning technique that just ‘works’. I find that most dosimetrists have their technique they swear by, but it may not work for everybody or every patient. We all have those special cases where the patient is unable to lie still for very long, or needs some sort of special accommodation. We also need to make sure that as dosimetrists, we are looking outside of our blinders from the plan in our treatment planning system and considering the needs of our therapists and most importantly, the patient.
Historically, when planning a hippocampal-avoidance whole brain, I would use multiple non-coplanar arcs to achieve the desired coverage and dose to the hippocampus. I had a technique that I thought was best and I still agree that it provides a very optimal dose distribution to the brain and proper sparing of organs including the hippocampus. All was good until I hit a road bump with a specific patient. This patient could not lie down on the table without becoming extremely nauseous. The patient did everything sitting up, even slept in a chair. Unfortunately, we had no way of treating a hippocampal-avoidance whole brain with a patient sitting up. We knew to treat this, there was no other option than to have the patient lie down. It was imperative to minimize the patient’s treatment time.
Simulation
During sim, the therapists staged and prepared as much as possible before the patient had to lie down on the table. They completed each task individually, allowing time for the patient to sit back up and gain composure. The mask was cut to allow part of the face to be exposed and the patient was eventually scanned with much discomfort and made it through the process.
Treatment Planning
In order to minimize the treatment time, I needed to develop a treatment plan which would minimize table time. I located a paper in the Medical Dosimetry journal from 2015 by Jin Shen, CMD et al titled An efficient Volumetric Arc Therapy treatment planning approach for hippocampal-avoidance whole-brain radiation therapy (HA-WBRT) which had a very unique approach that really ‘makes sense’ after reading it.
We all know the main goal of VMAT planning is to utilize the arc angles to treat the PTV while sparing the OARs as much as possible with sharp falloff. In order to achieve that, the paper describes how to utilize co-planar arcs with the jaws set so that the hippocampus is always near the edge of the jaw (above or below) so the leaves can consistently stay closed over the hippocampus. As the arc rotates, the section of PTV between the hippocampus is open for treatment delivery of dose and the leaves always remain closed over the organ at risk. The process is then repeated for the section remaining to be treated.
Historically, when planning a hippocampal-avoidance whole brain, I would use multiple non-coplanar arcs to achieve the desired coverage and dose to the hippocampus. I had a technique that I thought was best and I still agree that it provides a very optimal dose distribution to the brain and proper sparing of organs including the hippocampus. All was good until I hit a road bump with a specific patient. This patient could not lie down on the table without becoming extremely nauseous. The patient did everything sitting up, even slept in a chair. Unfortunately, we had no way of treating a hippocampal-avoidance whole brain with a patient sitting up. We knew to treat this, there was no other option than to have the patient lie down. It was imperative to minimize the patient’s treatment time.
Simulation
During sim, the therapists staged and prepared as much as possible before the patient had to lie down on the table. They completed each task individually, allowing time for the patient to sit back up and gain composure. The mask was cut to allow part of the face to be exposed and the patient was eventually scanned with much discomfort and made it through the process.
Treatment Planning
In order to minimize the treatment time, I needed to develop a treatment plan which would minimize table time. I located a paper in the Medical Dosimetry journal from 2015 by Jin Shen, CMD et al titled An efficient Volumetric Arc Therapy treatment planning approach for hippocampal-avoidance whole-brain radiation therapy (HA-WBRT) which had a very unique approach that really ‘makes sense’ after reading it.
We all know the main goal of VMAT planning is to utilize the arc angles to treat the PTV while sparing the OARs as much as possible with sharp falloff. In order to achieve that, the paper describes how to utilize co-planar arcs with the jaws set so that the hippocampus is always near the edge of the jaw (above or below) so the leaves can consistently stay closed over the hippocampus. As the arc rotates, the section of PTV between the hippocampus is open for treatment delivery of dose and the leaves always remain closed over the organ at risk. The process is then repeated for the section remaining to be treated.
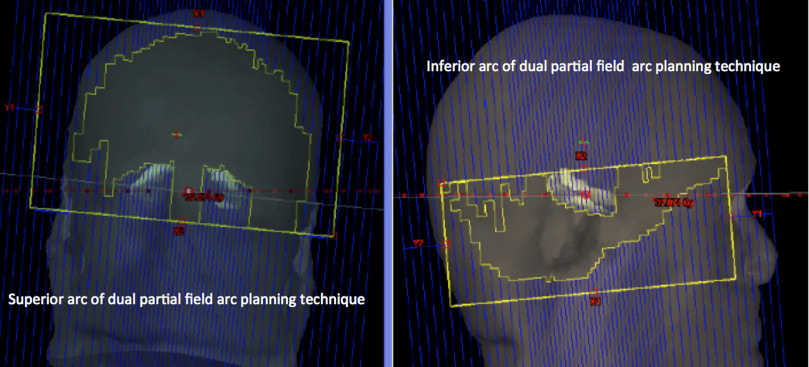
Fig. 4 from An efficient Volumetric Arc Therapy treatment planning approach for hippocampal-avoidance whole-brain radiation therapy (HA-WBRT)
Using this technique helped to develop a treatment plan to remove the extra time moving the couch during treatment. It also allowed the treatment plan to pass all RTOG 0933 constraints.
Treatment
The physician prescribed anti-nausea medication for the patient to take before treatments. The patient was uncomfortable, but was able to make it through the treatments. We estimated that about two minutes of time was removed from the total time the patient was on the table, which was a significant improvement in the care and comfort of this specific patient.
Using this technique helped to develop a treatment plan to remove the extra time moving the couch during treatment. It also allowed the treatment plan to pass all RTOG 0933 constraints.
Treatment
The physician prescribed anti-nausea medication for the patient to take before treatments. The patient was uncomfortable, but was able to make it through the treatments. We estimated that about two minutes of time was removed from the total time the patient was on the table, which was a significant improvement in the care and comfort of this specific patient.